Actinomycosis
Thoracic actinomycosis is a chronic suppurative pulmonary or endobronchial infection caused by Actinomyces israelii,
a gram-positive anaerobic saprophytic orgamism in the oral cavity.
Actinomycosis typically follows aspiration of endogenous organisms of the oropharynx into the lungs in people with poor oral hygiene or from extension of cervicofacial infections.
Confirmative diagnosis: histopathology
- Histopathologic findings of Actinomyces colonies or sulfur granules (yellowish aggregates of clustered mycelia)
- Filamentous structures within the tissue specimen positive for Grocott-Gomori methenamine-silver staining
CT findings
- Typical findings: chronic segmental air-space consolidations that contain low-attenuation areas with frequent cavity formation and peripheral enhancement,
and adjacent pleural thickening
- Central low attenuation: microabscess or necrotic material contained within ectatic bronchi
- Peripheral enhancing portion: chronic inflammation with a varying degree of fibrosis
- Consolidation is usually segmental in distribution at the time of diagnosis,
it can replace a whole lobe at a later stage and sometimes can cross the adjacent interlobar fissure.

Fig. 1: Contrast enhanced CT image obtained with mediastinal window setting shows subsegmental consolidation containing low attenuation area with peripheral enhacenment in the lingular segment of the left upper lobe and adjacent pleural thickening.
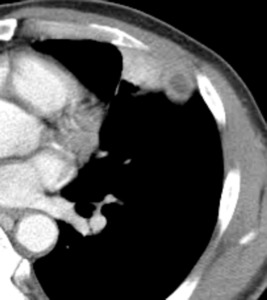
Fig. 2: Contrast enhanced CT image obtained on a lower level than A shows small subpleural nodular consolidation with central low attenuation and peripheral enhancement.

Fig. 3: Photomicrograph of specimen obtained through wedge resection shows colonies of actinomyces.
Paragonimiasis
Pleuropulmonary paragonimiasis is a food-borne parasitic disease caused by the lung fluke Paragonimus westermani,
which is endemic in Southeast Asia and the Far East.
Human infections occur when raw or incompletely cooked freshwater crabs or crayfish infected with metacercariae are ingested.
Diagnosis
- Detection of parasite eggs : sputum,
specimens of surgical excision or transthoracic needle aspiration biopsy
- Immunoserologic test : ELISA (+)
CT findings
- Early findings:
- pneumothorax or hydropneumothorax: caused by pleural penetration of worms
- focal air-space consolidation: juvenile worms migrate within the lung,
causing focal hemorrhagic pneumonia
- linear opacities: worm migration tract or peripheral atelectasis caused by small airway obstruction by the worm or egg granuloma
- Later findings:
- thin-walled cysts: the juvenile worms migrate within the lung until the settle,
forming a cyst around them
- dense masslike consolidation,
nodules,
or bronchiectasis

Fig. 4: Axial contrast-enhanced CT scan at mediastinal window setting shows subpleural nodular consolidation containing low attenuation in the right lower lobe with a broad base on the pleura. And there was diffuse thickening of the pleura and pleural effusion in the right lower hemithorax.

Fig. 5: CT scan at lung window setting shows linear structure that suggests worm migration tracts.

Fig. 6: Photomicrograph of specimen obtained wedge resection shows ‘worm cysts’(arrowheads, abscess cavities, small groups of paragonimus eggs within the lung tissue, where necrosis and the formation of a fibrous capsule) including several paragonimus eggs in the chronic inflammatory granulation tissue.
Pulmonary tuberculosis
Pulmonary tuberculosis is characterized histopathologically by caseating graulomas or pneumonia in the active phase and fibrosis and dystrophic calcification ininactive phase.
(1) Primary tuberculosis
Primary tuberculosis is seen in patients non previously exposed to M tuberculosis.
It is most common in infants and children and has highest prevalence in children under 5 years of age.
Radiologic findings
- Dense,
homogeneous well-defined segmental or lobar consolidation in any lobe (however,
predominance in the lower and middle lobe)
- Enlargement of lymph node in the hilum or the mediastinum.
(2) Postprimary tuberculosis
Postprimary tuberculosis occurs in patients previously sensitized to M tuberculosis.
Radiologic findings
- Most commonly involves the apical and posterior segments of the upper lung lobes and the superior segments of the lower lobes
- Centrilobular nodules and branching linear structures,
giving a tree-in-bud appearance
- Lobular consolidation
- Cavitation
- Bronchial wall thickening
- tuberculomas
round or oval granulomas with a regular and smooth outline (also spiculated margin)
surrounding satellite nodules,
and internal cavitation
ring-like or central curvilinear enhancement

Fig. 7: Contrast enhanced CT image shows subpleural mass-like consolidation containing clustered low attenuated areas, with lobulated margin and adjacent pleural effusion.

Fig. 8: Contrast enhanced CT image obtained on a upper level shows small subpleural nodule with an adjacent plerual thickening.

Fig. 9: Lung window setting shows centrilobular nodules around the nodule.
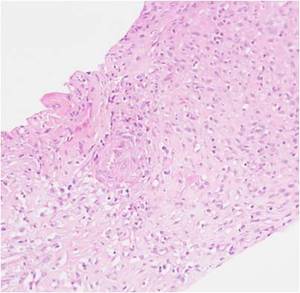
Fig. 10: Photomicrograph of histopathologic specimen shows tuberculoid granulomatous inflammation with necrosis.
Aspergillosis
Aspergillosis is a mycotic disease caused by Aspergilus organisms and frequently seen in immunocompromised patients.
Pulmonary aspergillosis can be subdevided into five categries:
- Saprophytic aspergillosis (aspergilloma)
- Hypersensitivity reaction (allergic bronchopulmonary aspergillosis)
- Semi-invasive (chronic necrotizing aspergillosis)
- Airway-invasive aspergillosis
- Angioinvasive aspergillosis
Histopathology
- invasion and occlusion of small to medium-sized pulmonary arteries by fungal hyphae
Radiologic findings
- nodules surrounded by a halo of ground-glass attenuation (“halo sign”) or pleura-based,
wedge-shaped areas of consolidation,
which are correspond to hemorrhagic infarcts.

Fig. 11: CT scan at lung window setting image shows subpleural mass-like consolidation in the right lower lobe.

Fig. 12: CT image obtained on an upper level shows internal cavitation and halo of ground-glass attenuation.

Fig. 13: High-power photomicrograph shows aspergillus hyphae, which are septate and have a fairly uniform thickness, and branch dichotomously.
Cryptococcosis
Cryptococcus neoformans is a thin-walled,
nonmycelial,
budding encapsulated yeastlike fungus.
It is found worldwide,
particularly in soil contaminated with pigeon excreta and decayed wood.
Human infection occurs via inhalation of cryptococcal particles into the lungs
Pathologic diagnosis
Mucicarmine stain
- Strong positive (bright red),
mucinous yeast capsule
Methenamine silver stain
- Yeast forms with no evidence of budding
PAS stain
- Pale round structure of organism
Imaging findings
- Single or multiple pulmonary nodules (5~52mm) peripherally located
- Focal areas of consolidation
- Small nodular or reticulonodular opacities
Immunocompetent patient
- Nodular consolidations
Immunocompromised patient
- Miliary pattern,
cavitation,
pleural effusion, lymphadenopathies
- Extrathoracic dissemination to brain and meninges

Fig. 14: CT scan at lung window setting image shows subpleural nodular consolidation and several peripheral nodules in the left lower lobe.

Fig. 15: CT scan at lung window setting image shows subpleural nodular consolidation and several peripheral nodules in the left lower lobe.

Fig. 16: CT image obtained with lung window setting at same level after antibiotics therapy shows an increased size of the nodular consolidation with newly developed internal cavitation.

Fig. 17: High-power photomicrograph shows fungal spores among the inflammatory cells.
Septic embolism
Septic embolism is nonthrombotic pulmonary embolism,
originated from septic phlebitis (purulent material mixed with fibrin thrombus) at primary site of infection
Common predisposing factors
- Tricuspid valve endocarditis with or without drug addiction
- Alcoholism
- Skin infection
- Immunologic deficiencies (particularily lymphoma)
Radiologic findings
- Discrete nodules with varying degrees of cavitation and most numerous in the lower lobes
- Subpleural,
wedge shaped heterogenous areas of increased attenuation
- Feeding vessel sign: a vessel can be seen leading directly the nodules

Fig. 18: CT scan at lung window setting image shows cavitating nodular consolidation with a distinct central vessel leading into it.

Fig. 19: Mediastinum window setting shows poor enhancement of the subpleural nodular consolidation.
Differential diagnosis
- The typical findings of Actinomycosis are chronic segmental air-space consolidation that contain low-attenuation areas with peripheral enhancement and adjacent pleural thickening.
- Pulmonary infiltration of Paragonimiasis are usually ill defined consolidations that change with time and accompany linear opacities or thin walled cyst adjacent to the consolidation and pneumothorax or hydropneumothorax.
-
If CT findings of tuberculosis show only subpleural consolidation,
it is difficult to differentiate with other infectious diseases.
But most of them show low attenuation or cavitation with smooth or spiculated margin and accompanied with centrilobular nodules or bronchial wall thickening.
-
If the CT findings in immumocompromise patients shows peripheral nodule or consolidation with perilesional ground glass attenuation,
you must consider fungal infection.
- The CT findings of septic embolism which usually develop in the lower lobe are discrete nodules with varying degrees of cavitation,
subpleural wedge shaped heterogenous areas of increased attenuation and feeding vessel signs may be shown.
-
The various infectious diseases described above occur in different areas of the lung along with the subpleural area.
But paragonimiasis and septic embolism usually occur in the subpleural area.
-
Though these lesions accompany internal low attenuation areas and various levels of peripheral enhancement,
less enhancement is shown in aspergillosis and septic embolism.






